

Who is Saturn Pathology?
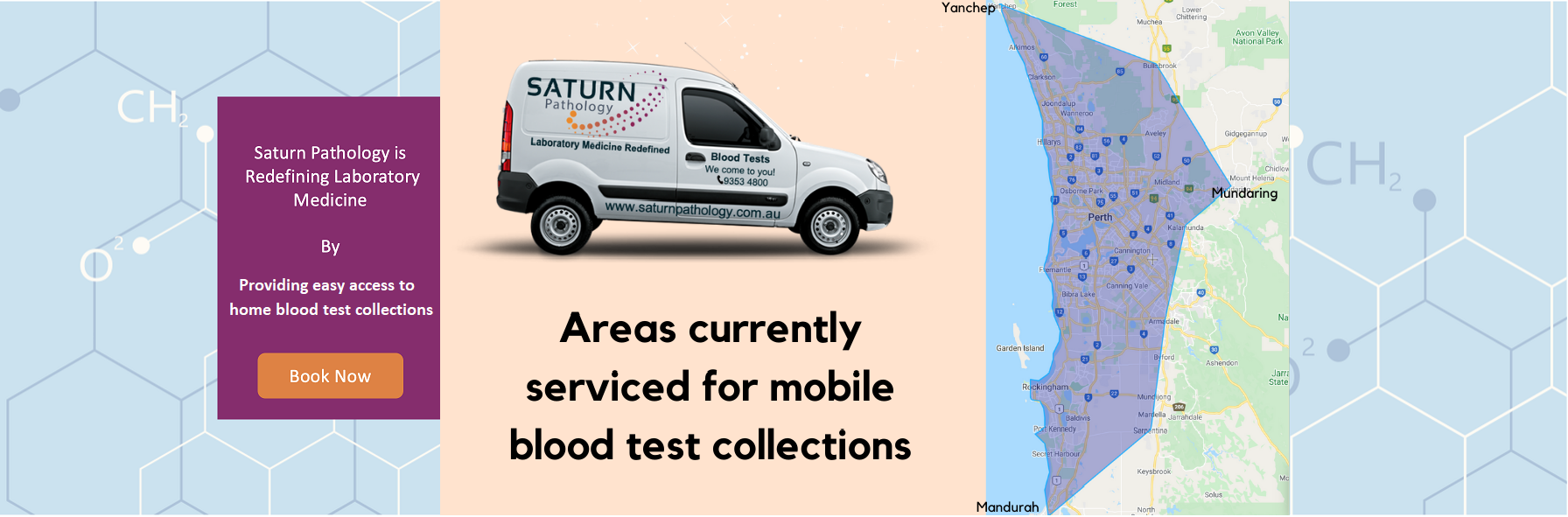
Saturn Pathology is a certified Western Australian medical laboratory that offers mobile appointment based blood test collections.

Patient
Saturn Pathology has put you at the centre of our business.
We provide a convenient home customised blood testing service, where our highly qualified collectors will come to you.
You can Request an Appointment (via Book Now) or SMS Request Form photos to 0456-SATURN or 0456-728876

Clinician
Saturn Pathology is all about service.
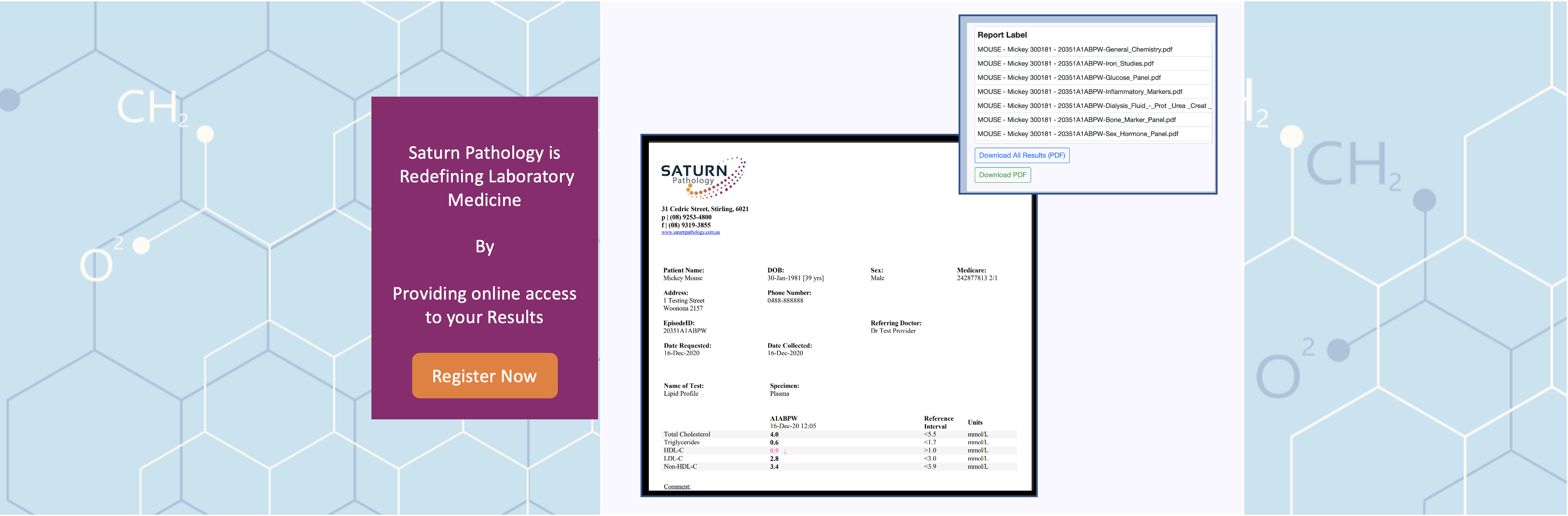
From easy online ordering and results to friendly accessible pathologists, we are here when you need us.

Our team is ready when you are.

We understand that children are not just little adults.

Our friendly Pathologists are looking forward to assisting you.